로봇 갑상선수술 중 신경모니터링
Intraoperative neuromonitoring during robotic thyroidectomy
Article information

Trans Abstract
Robot-assisted thyroidectomy (RAT) offers superior cosmetic outcomes and precise surgical control, but remote approaches pose unique risks of recurrent laryngeal nerve and external branch of the superior laryngeal nerve injury. This review summarizes the role of intraoperative neuromonitoring (IONM) in RAT, focusing on stimulation protocols, endotracheal tube positioning, and continuous neuromonitoring for early traction injury detection. Literature demonstrates that IONM improves functional nerve preservation, assists surgical decision-making, and enhances safety, particularly in transaxillary and transoral approaches. IONM contributes not only to intraoperative nerve preservation but also to safer surgical learning curves and standardized decision-making in robotic thyroidectomy.
서론
로봇 갑상선수술(robot-assisted thyroidectomy)은 기존 경부 절개 수술 대비 우수한 미용적 결과와 고배율의 안정된 3차원 시야, 정교한 다관절 기구 조작이 가능하다는 장점으로 아시아를 중심으로 널리 확산되었다[1]. 특히 경부 흉터에 대한 심리적 부담이 큰 젊은 여성 환자에서 높은 선호도를 보이며, 국내에서도 다양한 원위부 접근법(경액와[transaxillary], 후이개[retroauricular], 경구강전정[transoral vestibular])이 표준 수술 옵션으로 자리잡고 있다[2]. 그러나 원위부 접근 방식은 긴 수술 경로, 제한된 촉지(palpation)의 부재, 수술 기구의 레버리지 및 traction에 의한 시야 확보 필요 등으로 인해 반회후두신경(recurrent laryngeal nerve, RLN) 및 상후두신경 외지(external branch of the superior laryngeal nerve, EBSLN) 손상 위험이 존재한다[3,4]. 신경 손상은 음성 변성, 연하곤란, 기도 보호 저해 등의 기능적 장애를 초래하며 환자의 삶의 질에 큰 영향을 끼친다[5].
수술 중 신경모니터링(intraoperative neuromonitoring, IONM)은 이러한 위험을 낮추기 위한 중요한 보조 기술로, 신경의 해부학적 위치 확인뿐만 아니라 실시간 기능 평가가 가능하다[6]. 개방 갑상선수술에서 이미 그 효과가 입증되었으며, 로봇수술의 고유한 기계적⋅시야적 제한 요소를 극복하기 위해 필수적인 도구로 평가받는다[7]. 또한 최근에는 traction injury 예방을 위한 연속 신경감시(연속 수술 중 신경모니터링, continuous IONM [C-IONM]) 및 신호 패턴 분석을 기반으로 한 연구가 활발히 이루어지며, 로봇수술 환경에 최적화된 IONM 전략 필요성이 더욱 강조되고 있다. 본 연구는 최신 문헌 고찰을 통해 로봇 갑상선수술에서 IONM의 임상적 역할, 적용 방법 및 향후 발전 방향을 기술하고자 한다.
방법
본 연구는 로봇 갑상선수술에서 IONM의 적용과 임상적 유용성을 평가하기 위한 서술적 문헌 고찰 연구이다. PubMed, Scopus, Web of Science, KoreaMed, RISS를 포함한 주요 데이터베이스를 이용하여 2009년 1월부터 2024년 12월까지 발표된 문헌을 검색하였다. 검색어로는 “robotic thyroidectomy”, “remote-access thyroid surgery”, “recurrent laryngeal nerve monitoring”, “continuous IONM”, “EBSLN monitoring”, “TOETVA”, “transaxillary approach” 등을 사용하였다. 원위부 접근 로봇수술(transaxillary, retroauricular, transoral vestibular)에서 IONM이 적용된 임상 연구, 후향적 분석, 전향적 연구, 메타분석, 국제 가이드라인을 포함하였다. 원래 원저와 메타분석을 포함하여 총 62개 연구가 포함 기준을 충족했지만 수술 후 음성과 근전도(electromyography, EMG) 데이터가 부족하여 14개 논문이 제외되었다.
선정 기준은 (1) 로봇 갑상선수술 시행, (2) RLN 또는 EBSLN 모니터링 수행, (3) 수술 후 성대 기능 또는 EMG 소견 보고가 포함된 경우로 하였다. 증례 보고(single case report), 실험실 동물 모델, 음성 결과가 보고되지 않은 기술 보고는 제외하였다. 또한 로봇 수술 도입기 초반 논문 중 술자 경험이 10예 이하인 경우는 학습곡선 영향 배제를 위해 제외하였다. 각 문헌에서 IONM 프로토콜(V1–R1–R2–V2), EMG 진폭 및 잠복기 변화 기준, C-IONM 여부, 신경 손상률, 음성 평가 도구(Voice Handicap Index, stroboscopy) 등을 분석하였다.
1. Quality appraisal
본 논문은 서술적 문헌 고찰로서 체계적 품질평가(공식 sisk of bias [RoB] 도구)는 수행하지 않았으며, 동료심사된 임상 연구와 가이드라인을 우선 포함하되 원문에서 보고된 RoB (무작위연구의 RoB-2, 비무작위연구의 ROBINS-I)가 있는 경우 이를 참조하였다.
고찰
로봇 갑상선수술은 경부 절개를 회피하면서 우수한 시야와 정밀한 기구 조작을 제공하나 긴 접근 경로와 해부학적 지표의 변화로 인해 신경 손상 위험이 존재한다[3]. 특히 경액와(transaxillary)와 경구강(transoral vestibular) 접근은 수술 기구의 움직임에 따른 traction, 열 손상, 그리고 기도 튜브 위치 변화에 따른 EMG 접촉 불량이 주요 위험 요소로 보고된다[4,8]. 이러한 한계 속에서 IONM은 신경의 실시간 기능 정보를 제공하여 손상 예방에 중요한 역할을 한다.
IONM의 핵심 기전은 RLN 및 미주신경에 전기 자극을 가하여 EMG 반응을 측정함으로써 신경의 기능적 상태를 파악하는 것이다. 국제 표준 프로토콜(V1–R1–R2–V2) 적용을 통해 수술 시작 전과 후의 신경 상태를 비교할 수 있으며, 이는 traction injury, thermal injury, clamping injury 등 다양한 기전의 신경 손상을 조기에 감지하는 데 도움을 준다[6]. 특히 로봇 수술에서는 수술 기구가 좁은 공간에서 장시간 traction을 유지하는 경우가 많아 신경의 신전 및 허혈에 의한 기능 저하가 발생할 수 있는데, IONM은 이러한 변화를 즉각 반영한다[9].
C-IONM은 최근 점차 도입되고 있으며, RLN의 지속적인 자극을 통해 EMG 변화(진폭 50% 이상 감소, 잠복기 10% 이상 지연)를 조기에 탐지하여 즉시 수술 전략을 조정할 수 있다. 특히 경구 내시경 갑상선 절제술(transoral endoscopic thyroidectomy vestibular approach)에서는 기도 튜브의 회전, 로봇 팔의 충격(clashing), 흡인기 음압 등에 의해 EMG 접촉이 불안정해질 가능성이 높아 C-IONM이 안정성을 높이는 역할을 한다고 보고된다[8]. 또한 C-IONM이 traction injury 예방에 기여할 수 있음을 제시하고 있다[10].
최근 연구들은 로봇 갑상선 절제술에서 C-IONM의 보호적 역할을 뒷받침하고 있다. 여러 연구들에서 C-IONM을 적용했을 때 로봇 수술군에서 일시적 성대마비 발생률이 낮았다고 보고했으며[9], 로봇 갑상선 절제술과 고식적 갑상선 절제술 간에 IONM의 효능이 유사함을 확인하여 원격 접근 수술 시 신경 보존에 있어 IONM의 가치를 강조했다.
그러나 IONM이 신경 손상률을 절대적으로 감소시키는지에 대해서는 일부 이견이 있다. 이는 술자 경험, 장비 세팅, 튜브 위치 조절, 해부학적 변이에 따른 차이가 복합적으로 작용하기 때문이다. 특히 C-IONM이 최적의 예방효과를 발휘하기 위해서는 EMG 파형의 품질 유지가 필수이며, 수술 중 anesthesia depth control과 neuromuscular blockade reversal 등 마취 협업이 중요하다. 또한 로봇 수술에서 발생할 수 있는 기구 관련 artifact, energy device 사용 시 baseline noise 상승 등 기술적 한계도 존재한다(Table 1).
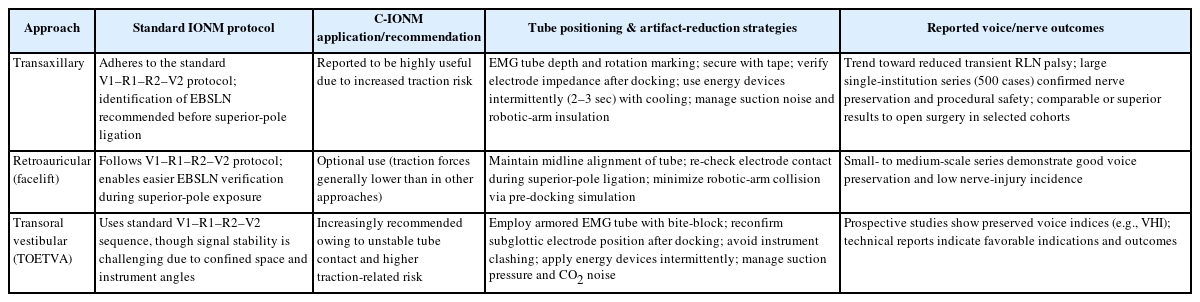
Summary of IONM application by robotic approach
그럼에도 불구하고, 현재까지의 근거는 IONM이 로봇 갑상선수술의 학습 곡선을 단축시키고 신경 손상 위험이 높은 경우에 유용하며, 특히 양측 갑상선 절제술을 고려하는 상황에서 환측 신경 기능 저하 시 반대측 수술을 연기해 영구적 양측마비를 예방하는 의사결정에 기여함을 보여준다. 향후 기술 발전 방향으로는 AI 기반 EMG 파형 분석, 로봇 시스템과의 직접 통합, traction force sensor를 이용한 자동 피드백 시스템 등이 제시되고 있다. 이러한 기술이 도입될 경우 RLN 보호 능력은 더욱 향상될 것으로 기대된다.
종합하면, IONM은 로봇 갑상선수술에서 신경 보존을 극대화하기 위한 필수적 보조 기술이며, 특히 원위부 접근 특성상 traction injury 위험이 높은 환자군에서 중요한 역할을 수행한다. 임상 적용 시 표준화된 술기 준수, 마취팀과의 협업, 장비 숙련, EMG 품질 유지 전략이 필수적이다.
결론
로봇 갑상선수술은 우수한 미용적 장점과 정교한 수술 시야를 제공하지만 원위부 접근에 따른 신경 손상 위험이 존재한다. IONM은 이러한 한계를 보완하여 RLN 및 EBSLN의 기능 보존을 돕고, traction 및 열 손상을 조기에 감지해 수술 전략을 적절히 조정할 수 있는 핵심 기술이다. 특히 연속 모니터링과 표준화된 프로토콜 적용은 신경 안전성을 강화하며, 술자의 학습 곡선을 단축하는 데에도 기여한다. 향후 AI 기반 EMG 분석과 로봇-통합형 모니터링 시스템 도입을 통해 신경 보호의 정확성과 자동화가 더욱 향상될 것으로 기대된다.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
None.
Author Contributions
Conceptualization: ESS; Investigation: JCL; Methodology: ML; Validation: ML; Writing–original draft: all authors; Writing–review & editing: all authors.