
서론
갑상선 수술 후 음성변화는 반회후두신경 (recurrent laryngeal nerve, RLN)과 상후두신경외분지 (external branch of superior laryngeal nerve, EBSLN)의 신경 손상에 의해 발생하는 경우와 신경의 손상 없이 후두 점막의 부종, 후두골격 주변의 근육과의 유착 등에 의해 발생하는 갑상선 수술 후 증후군 (post-thyroidectomy syndrome)으로 나누어 생각해 볼 수 있다[1]. 수술 후 성대마비가 없는 경우에도 30-87%의 환자에서 주관적인 음성 문제를 호소할 수 있으며, 다른 한편으로는 약 28%에서는 성대마비가 있어도 음성 문제를 호소하지 않을 수도 있다[2].
따라서, 각각의 경우를 잘 진단하고 적절하게 대처하는 것이 갑상선 수술 후 환자의 음성을 잘 보존하는 데 중요하다[2,3]. 본 종설에서는 갑상선 수술 후 발생할 수 있는 신경 손상을 비롯한 음성 손상 및 변화의 요인들과 각각의 경우, 이를 해결하기 위한 다양한 방법들에 대해 살펴보고자 한다.
반회후두신경
RLN 손상에 대한 수술 후 대응은 신경 손상이 영구적인지(갑상선 수술 중 RLN이 절제되어 신경 기능 소실이 발생할 것이 명백한 경우 등) 일시적인지에 따라 차이가 있을 수 있다. 즉, 외과의는 수술 중에 RLN, EBSLN에 대한 신경 모니터링을 통해 신경 기능에 대해 평가하는 것이 수술 후 환자 대응에 도움이 된다. 이 글에서는 영구적 신경 손상인 경우를 기준으로 기술하고자 한다.
신경재건술 (Reinnervation)
신경의 절단 및 절제가 발생하는 경우 단단문합술(end-to-end anastomosis), free nerve grafting, ansa cervicalis to RLN anastomosis, Vagus to RLN anastomosis 등의 방법으로 신경을 재건할 수 있다[4,5]. Ansa cervi-calis to RLN anastomosis의 경우 절제되는 신경의 크기가 비교적 긴 경우에도 사용될 수 있으며 수술 후 3-6개월에 걸쳐 음성의 개선을 확인할 수 있는 것으로 알려져 있다[4]. 갑상선암의 RLN 침범이 있어 신경을 절제해야 하는 경우에는 수술 전 성대마비 여부와 관계없이 신경 절제 후 reinnervation을 해 주는 것이 수술 후 환자의 음성을 개선하는 효과가 있으므로 가능하면 곧바로 시행하는 것을 고려한다[6,7]. 즉, 수술 전에 갑상선암의 RLN 침범으로 성대마비가 있는 환자에서도 수술 후 1년 째 유의한 음성개선이 확인되었으므로 적극적인 reinnervation이 필요하다[6].
성대주입술 (Injection laryngoplasty)
성대주입술을 위한 접근법으로는 cricothyroid approach, transcartilaginous approach, thyrohyoid ap-proach가 있으며 성대근육 내에 hyaluronic acid, cal-cium hydroxyapatite, autologous fat 등의 물질을 주입한다[8]. 성대주입술은 외래에서 국소마취 하에 시행될 수 있는 비교적 간단한 시술로서 즉각적인 음성개선을 확인할 수 있으며 일시적 성대마비로 예상되는 경우에도 많이 시행되고 있다. 일측 성대마비가 있더라도 음성 요구도가 낮거나 또는 흡인 위험이 적은 경우 6-12개월 정도는 경과 관찰해 볼 수 있다[3]. 그러나 , 갑상선 수술 후 성대마비시 조기에 성대주입술을 시행하는 것이 성대마비가 지속되는 경우에도 후두골격 수술(laryngeal framework surgery)이 요구되는 환자의 비율을 줄이는데 도움이 되는 것으로 보고되고 있다[9,10].
후두골격 수술 (Laryngeal framework surgery)
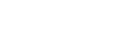
후두골격 수술은 성대마비가 발생한 후 수개월간 경과관찰 후 점막의 부종이 해소되고 근육의 위축이 발생한 후 시행하는 경우가 일반적이다[3]. 영구적인 성대마비로 판단될 경우, 내전 갑상성형술 (medialization thyroplasty)을 시행하여 성대를 내측으로 밀어주며 피열연골 내전술을 동시에 시행하여 마비된 성대 위치를 맞추어 주는 것이 좋다[11]. 내전 갑상성형술은 갑상연골에 창을 만들어 실리콘 블록, Gore-Tex strip, VoCom 등의 보형물을 삽입하는 방식이다 (Figure 1B) [12,13]. 피열연골 내전술은 피열연골의 근돌기 (muscular process)를 전방으로 당겨 피열연골을 내측으로 회전시킴으로써 성대를 내전시키는 원리로 음성을 개선시키다 (Figure 1C) [14]. 영구적인 성대마비 여부를 판단하기 어려운 경우, 성대마비 발생 6~12개월 후에 수술을 시행한다.
신경 도관 (Nerve guide conduit)
신경재생을 유도하기 위해 절단된 신경 사이에 도관 (conduit)을 삽입하여 신경이 정방향으로 합성될 수 있도록 유도하는 방법이다[15,16]. 신경도관은 내부가 비어 있는 튜브 모양으로 절단된 신경의 양측 사이 틈을 메우도록 디자인되어 있다. 최근 신경도관의 구조적 변경, 생체적합성 물질개발, 약물 방출 등을 활용한 조직 공학 기술이 다양하게 연구되고 있다. 이와 같은 신경 도관은 손상된 신경을 보호하면서 신경 성장인자나 생체활성 인자의 유입은 유지시키면서도 주변의 섬유화 조직의 침윤을 막아서 신경재생에 도움을 주는 것으로 보고되고 있다[16].
약물치료
성대마비 예방을 위해 전신 스테로이드를 일상적으로 주는 것은 근거가 부족하고 부작용의 위험이 있어 권고되지 않는다[20]. 그러나, 최근 Donatini 등에 따르면 수술 중 신경모니터링 중에 신호소실 (loss of sig-nal)일 발생하는 경우, 전신 스테로이드를 10분 내에 주사하면 영구적인 성대마비를 피하는데 도움이 된다고 보고되기도 했다[21]. 니모디핀 (Nimodipine)은 cal-cium channel blocker로 고혈압 및 지주막하출혈 후 혈관연축 (vasospasm)을 예방하는 목적으로 사용되어 왔다. 최근 한 메타분석에 따르면 RLN 손상으로 성대마비가 발생한 환자에서 니모디핀을 투여한 군에서 기능 회복의 odds ratio가 13.73로 보고 되었다[22]. 명확한 작용 기전은 아직 알려져 있지 않으나 니모디핀이 손상된 신경의 axon 성장을 촉진시키는 것이 확인된 바 있다[23]. 연구자에 따라 사용 용량은 다른데 1일 30 mg, 3회부터 60 mg, 6회 등 다양하게 투약하고 있다[22]. 임신 및 수유 중인 경우, 심혈관계 질환이 있는 경우 등 약물 처방의 적응증에 해당하지 않은 경우 등이 있으므로 주의를 요하며[22] 어지러움, 두통 등의 부작용으로 약물을 중단하는 경우도 29%에 이른다는 보고가 있다[23].
양측 성대 마비의 치료
양측성 성대마비가 발생하면 수술 후 호흡곤란이 발생할 있으며 흡인을 동반한 연하곤란이 발생할 수 있다. 필요에 따라 기관절개술, 경구강 레이저를 이용한 posterior cordotomy, vocal fold lateralization, arytenoid abduction, Botox injection 등을 시행할 수 있다[24].
상후두신경의 외분지
윤상갑상근을 지배하는 EBSLN 손상시 고음장애를 비롯한 음성장애가 발생할 수 있다. 음성치료를 통해 muscle tension dysphonia로 진행되지 않도록 음성치료를 받는 것이 좋다. 최근 Miyauchi 등은 ansa cervical - EBSLN anastomosis를 통해 수술 중 손상된 EBSLN을 재건하는 방법에 대해 보고하였는데 수술 5개월 후 음성이 개선되는 결과를 보였다고 한다[5].
갑상선 수술 후 증후군
갑상선 수술 후 RLN, EBSLN의 명백한 손상은 확인되지 않지만 환자가 음성장애나 연하장애를 호소하는 경우가 있는데, 이를 갑상선 수술 후 증후군이라고 한다[1,3]. 갑상선 수술 후 증후군이 발생하는 원인으로는 윤상갑상근 손상, 피대근을 비롯한 후두 주변 조직의 손상과 유착, 후두의 혈액순환장애, 기관 삽관시 외상, 수술에 의한 심리적 영향 등이 있을 수 있다[1].
수술 후 후두기관의 유착을 최소화하기 위해 수술 다음 날부터 경부 운동을 시행하는 것이 도움이 된다고 알려져 있다. 경부 불편감, 경부 운동 범위 등에도 유의한 호전을 관찰할 수 있다고 한다. 더불어, 음성위생에 대한 교육과 함께 relaxation & breathing exercise, laryngeal massage, resonance therapy, digital com-pression 등의 음성 치료가 다양한 음성 지표의 호전을 보였다는 보고들도 있다. 수술 후 조기에 음성치료를 시행하는 것이 향후 음성 결과와 삶의 질 향상에 도움이 된다고 보고되고 있다.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




