갑상선 수술 중 신경감시 없이 상후두신경 보존하는 방법
Preservation of the superior laryngeal nerve without neuromonitoring during thyroid surgery
Article information

Trans Abstract
Recently, Intraoperative neurophysiological monitoring (IONM) has enabled the prevention of nerve injury, reducing the incidence of complications associated with nerve injury even in high-risk surgeries. However, reliance on IONM is not feasible in all situations. Therefore, surgeons have the necessity and obligation to master the techniques for identifying and preserving nerves without the aid of neurophysiological monitoring. Therefore, it aims to introduce the course and variations of the superior laryngeal nerve, as well as methods for identifying and preserving the external branch of the superior laryngeal nerve during thyroid surgery without the use of intraoperative neurophysiological monitoring.
서론
갑상선 수술 과정에서 가장 중요한 과정은 반회후두신경(recurrent laryngeal nerve)과 상후두신경의 외측분지(external branch of superior laryngeal nerve)의 보존일 것이다. 이 두 신경은 발성에 관여하는 운동신경으로 손상 시 일상 생활에 지장을 주어 삶의 질 저하를 초래할 수 있어 수술 시 신경을 보존하는 것은 매우 중요하다. 최근 수술 중 신경감시(intraoperative neuro-physiological monitoring, IONM)의 보급으로 신경 손상을 예방할 수 있게 되었고 신경 손상의 가능성이 높은 고위험군의 수술에서도 신경 손상의 합병증을 감소시킬 수 있게 되었다. 하지만 모든 상황에서 신경감시 장치에 의존할 수는 없기에, 외과의라면 신경감시 없이 신경을 확인하고 보존하는 술기를 숙지해야 할 필요와 의무가 있다.
상후두신경 외측분지는 보고자마다 차이가 있으나 일반적으로 반회후두신경보다 신경 손상 비율이 높다고 알려져 있다. 반회후두신경 마비율은 4% 정도로 보고되고 있으나 상후두신경 외측분지는 0.4-58%로 다양하게 보고되고 있다[1-3]. 이는 몇 가지 이유가 있는데 상후두신경 외측분지는 갑상선 상극주변에서 주행하므로 수술 시야가 충분히 확보되지 않는 점, 신경 주행의 변이가 많아 육안으로 확인이 쉽지 않은 점, 그리고 상후두신경 외측분지는 고음 발성에 관여하므로 일상적인 발성에는 지장이 없어 상대적으로 반회후두신경에 비해 관심도가 낮아 신경 손상 평가가 부정확하게 이루어지거나 누락되는 점 등을 들 수 있다[4-7].
최근 고음 발성에 대한 관심이 높아지는 경향이 있고 직업적으로 고음 발성이 중요한 환자들도 많기에 수술 시 반회후두신경 못지 않게 상후두신경을 잘 보존하는 것이 중요하다[4-9]. 이에 상후두신경의 주행 경로 및 변이, 갑상선 수술 시 상후두신경을 보존하는 방법을 알아보고자 한다.
상후두신경 외측분지의 주행
상후두신경의 외측분지는 상갑상동맥과 정맥을 따라 하인두 수축근 표면을 타고 내려오며 갑상선 상극 주변에서 윤상갑상근을 향해 주행한다. 수술 시야에서 는 흉골갑상근(sternothyroid muscle)을 앞쪽 경계로, 이 근육을 견인하면 하인두 수축근을 내측 경계로 하고 갑상선 상극과 상갑상혈관을 외측 경계로 하며 윤상갑상근을 바닥으로 하는 가상의 삼각형 공간을 상정할 수 있고 이 공간으로 상후두 신경의 외측 분지가 지나가는 것을 확인할 수 있다. 이 공간을 흉골갑상-후두 삼각(sternothyroid-laryngeal triangle) 또는 Joll’s tri-angle이라고 칭한다.
상후두신경 외측분지의 변이
상후두신경 외측분지의 주행 경로의 변이에 대한 다양한 분류법이 있으나 대표적인 3가지 분류법을 소개하고자 한다[2,10-12].
Cernea Classification
상후두신경이 상갑상혈관과 교차하는 위치에 따른 분류법으로 다음과 같다.
제 1형 : 갑상선 상극의 꼭대기 부분에서 1cm 이상 상부에서 상갑상혈관을 교차하여 주행하며 작은 갑상선종 환자의 68%, 큰 갑상선종의 23%에서 나타난다.
제 2-A형: 갑상선 상극 꼭대기 부분에서 1cm 미만의 거리에서 상갑상혈관과 교차하여 주행하며 작은 갑상선종 환자의 18%, 큰 갑상선종의 15%에서 나타난다.
제 2-B형: 갑상선 상극 경계보다 아래에서 상갑상혈관을 교차하여 주행하며 작은 갑상선종 환자의 14%, 큰 갑상선종 환자의 54%에서 나타난다.
1형 보다 2형이, 2형 중에서는 2-B형이 수술 중 신경 손상의 확률이 높다.
Kierner Classification
Cernea 분류법과 유사하며 1형에서 3형까지는 Cernea 분류의 1형, 2-A형, 2-B형과 동일하며 갑상선 상극의 꼭지점 부근 직상방에서 상갑상혈관의 배면(dorsal)으로 교차하는 것(4)형 을 추가하여 총 4가지 형태로 분류하였다.
Friedman Classification
상후두신경이 하인두 수축근의 표면 위로 주행하는 것이 일반적으로 알려져 있는 주행인데 하인두 수축근 내로 주행하는 변이가 있어 이에 대한 분류를 한 방법이다.
제 1형: 하인두 수축근 표면 위에서 주행하며 약 50%에서 나타난다.
제 2형: 윤상갑상근 근위부 1cm에서 하인두 수축근 내부로 들어가서 주행한다.
제 3형: 하인두 수축근 내부에서 주행하며 약 15%로 가장 적은 빈도에서 발견된다.
수술 중 상후두신경을 보존하는 방법
상후두신경을 육안으로 확인하는 방법
하인두 수축근 박리
대부분 하인두 수축근 표면으로 신경이 주행하므로 하인두 수축근을 찾고 주변을 박리하여 육안으로 상후두신경을 확인한다. 단 Friedman 분류에서도 확인할 수 있듯이 신경 주행 경로의 변이가 있거나 박리 과정에서 섬세하지 못한 경우 오히려 신경 손상이 발생할 수 있다는 것을 주의해야 한다.
피대근 견인 / 제거
대부분의 갑상선 수술은 최대한 보존적으로 이루어지기 때문에 가급적 주변 구조물을 보존하면서 진행한다. 갑상선 수술 시 상극 주변의 구조물은 시야가 제한적인 경우가 많고 피대근이 그 장애물 중에 하나인 경우가 많아 견인을 충분히 하더라도 시야가 제한적이라면 피대근을 제거하여 시야를 충분히 확보해 준다. 이에 더불어 신경 주행의 경로 및 해부학적 지표 등을 참고 삼는다면 신경을 육안으로 확인하는데 도움이 된다(Figure 1).
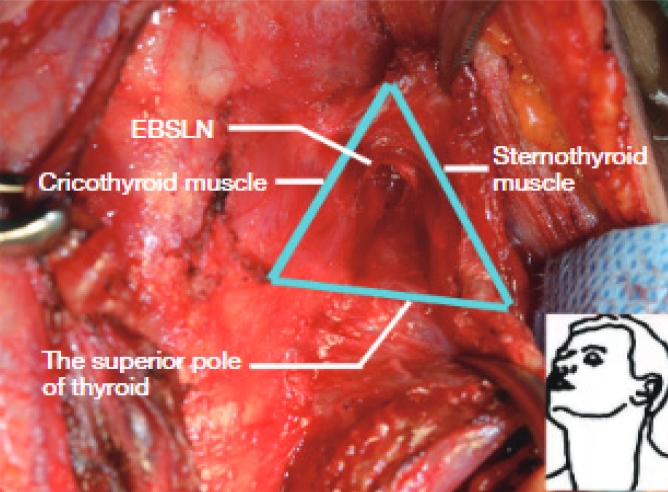
Joll’s triangle. External branch of superior laryngeal nerve (EBSLN) is identified in the anatomical landmark.
역행성 갑상선절제술 (retrograde thyroidectomy)
역행성 갑상선절제술은 고식적 방법과 달리 협부(isthmus)를 절개 및 분리하는 과정을 시작으로 윤상기관 구조물(cricotracheal structure)과 갑상선 내측면 사이의 기관전근막(prevertebral fascia) 사이로 박리하며 진행한다. 이 과정에서 Berry 인대(가Berry’s ligament) 쉽게 노출된다. 흉골갑상근(sternothyroid muscle)과 갑상선 사이를 박리하고 하부갑상동맥 분지 결찰 및 하부부갑상선 확인 및 보존을 한 후 Zuckerkandl tubercle 내측에서 반회후두신경을 확인하고 보존한다. 이후 상부로 진행하며 Berry’s ligament를 분리하고 마지막으로 상갑상혈관을 결찰하며 갑상선 상극을 박리한다. 역행성 술기는 상후두신경의 외측분지를 확인하는 과정에서 갑상선 상극 주변의 시야 확보와 박리의 용이성 측면에서 신경 손상의 가능성을 감소시킬 수 있으며 Hur 등은 역행성 술기 시 상후두신경의 외측분지 손상은 1.7% 정도로 낮다고 보고한 바 있다[13-15].
상후두신경을 육안으로 확인하지 않고 보존하는 방법
신경 주변을 박리하는 과정에서 최대한 갑상선에 가깝게 박리하는 것이 중요하다. 최근에는 피막 박리(capsular dissection) 개념이 널리 통용되고 있으며, 이는 갑상동맥 3차 분지를 결찰하여 갑상선피막(capsular propria)과 기관전근막의 내장층(visceral layer of pre-tracheal fascia) 사이로 박리하여 부갑상선을 보존하는 술식이다[16,17].
상갑상혈관을 결찰하는 과정에서 최대한 갑상선 상극 피막에 가깝게 결찰하는 것이 상후두신경 손상을 줄일 수 있는 방법으로 Lekacos등은 이러한 방법으로 손상율를 0%까지 줄일 수 있다고 보고한 바 있다(Figure 2) [18,19]. 또한 갑상선의 상극 일부는 남기는 아전절제술(subtotal thyroidectomy)도 신경 보존을 위한 술식이 될 수 있다.
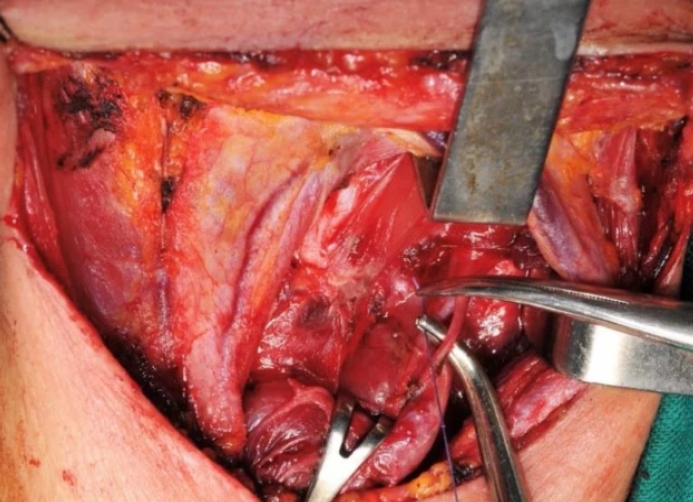
Ligation of superior thyroid artery (STA). STA division branches ligation performed as close to the thyroid gland as possible.
결론
상후두신경의 외측분지는 반회후두신경에 비해 찾기가 어렵고 변이도 많다. 그에 반해 신경 손상 시의 불편감은 반회후두신경 손상에 비해 크지 않아 그 중요성이 강조되지 않는 경향이 있다. 하지만 최근에는 고음 발성에 대한 관심과 중요성이 증가하고 있으며 주의를 기울이지 않으면 50% 이상에서 신경 손상이 발생할 수 있기에 갑상선 수술을 담당하는 외과의라면 반드시 상후두신경 외측분지를 확인하고 보존하려는 노력을 기울어야 한다. 신경감시 장치가 발전하고 보편화되고 있어 신경 손상의 빈도가 감소하고 있으나 오히려 이로 인해 외과의의 기술적 숙련도는 저하될 수도 있다는 점을 경계하며 신경 확인의 술기를 정확히 이해하려는 노력 또한 이루어져야 할 것이다.
Notes
Funding
None.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Data Availavility
None.